Facial Nerve (CN VII) Anatomy and Applied Surgical Anatomy of the Parotid Gland
Post date: 29/03/2026
For Medical Expert
Facial nerve: anatomy and surgical anatomy.
The facial nerve (CN VII) is a mixed nerve containing motor, sensory, and autonomic (parasympathetic) fibers. Its course is highly complex, extending from the brainstem, traversing the temporal bone, and terminating in the muscles of the face.
◦ Facial motor nucleus: Located in the pons. Motor fibers supply the ipsilateral muscles of facial expression (they do not decussate after leaving the nucleus).
◦ Superior salivatory nucleus and Lacrimal nucleus: Provide parasympathetic innervation.
◦ Sensory fibers for taste terminate in the solitary nucleus.
• Apparent Origin: The nerve emerges from the brainstem at the pontomedullary junction (bulbopontine sulcus).
• The facial nerve emerges as two roots: a large motor root located medially and a smaller intermediate nerve (CN VII') located laterally.
• In the posterior cranial fossa: From the brainstem, the nerve travels laterally and forward to reach the temporal bone.
• Internal acoustic meatus (IAM): The two roots of the facial nerve enter this opening along with the vestibulocochlear nerve (CN VIII) and the labyrinthine artery (which is a branch of the anterior inferior cerebellar artery - AICA).
• The blood supply to this region is provided by the labyrinthine artery.
Within the internal auditory meatus (IAM), the nervus intermedius merges with the motor root to establish a unified trunk. This combined facial nerve complex is situated in the anterosuperior quadrant of the meatus. Within this trunk, a specific orientation is maintained: the motor fibers are positioned anteriorly, while the nervus intermedius fibers lie posteriorly.
Anatomical Landmarks and Compartmentalization
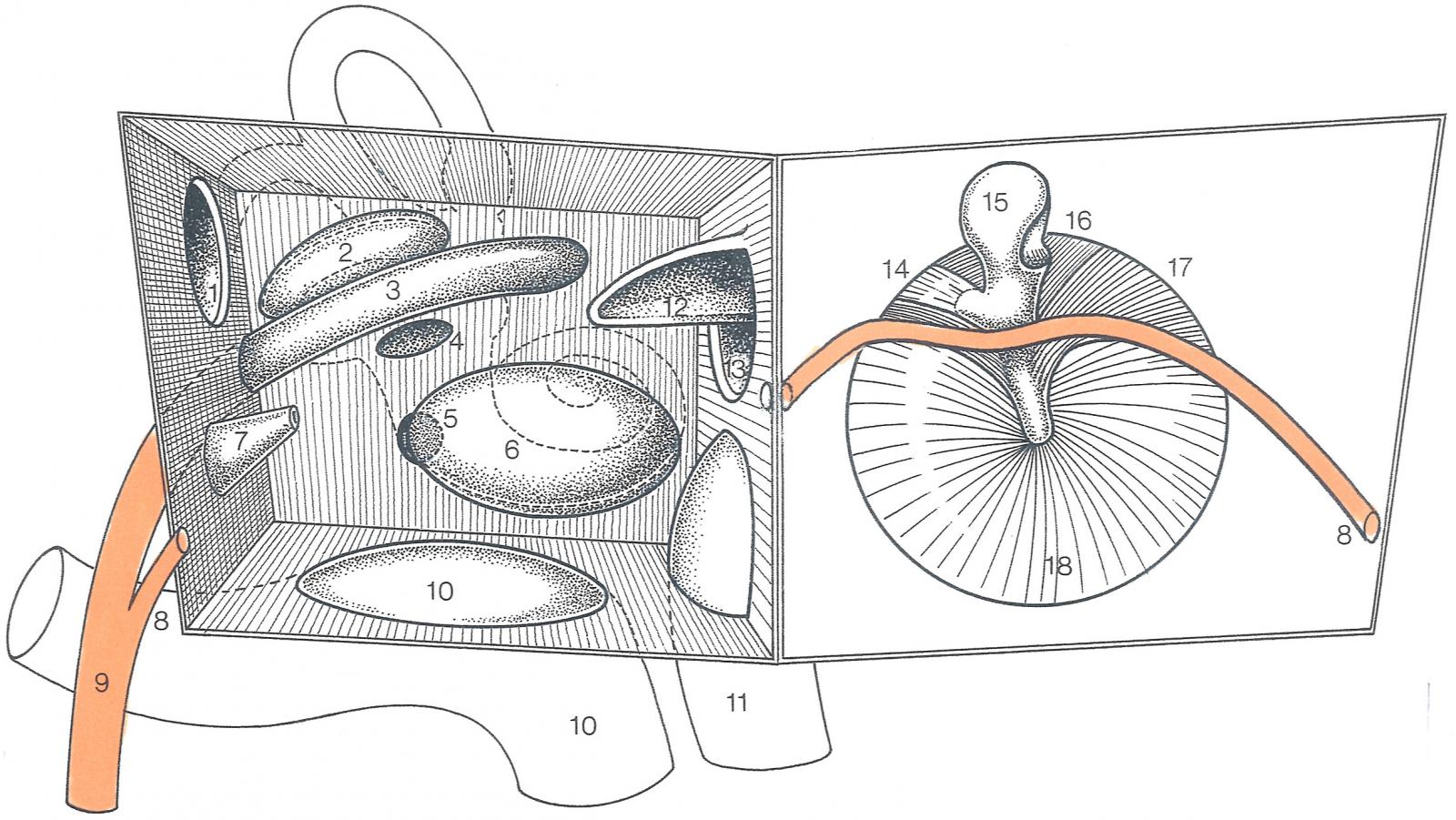
As the nerve reaches the lateral extremity (fundus) of the meatus, it is partitioned from adjacent cranial nerves by two distinct ridges:
• The Transverse (Falciform) Crest: A horizontal partition composed of dura and sometimes bone. It serves as the boundary separating the facial nerve (above) from the cochlear nerve (below).
• Bill’s Bar (Vertical Crest): An incomplete vertical ridge of bone and dura. This landmark separates the facial nerve (anteriorly) from the superior vestibular nerve (posteriorly).
image: internal acoustic meatus
Blood supply: labyrinthine artery - brand of the anterior inferior cerebellar artery.
• Genu of the Facial Nerve (First Genu): At the geniculate ganglion, the nerve makes a sharp, knee-like bend as it turns abruptly posterior.
• Tympanic Segment: Following the genu, the nerve creates a horizontal portion on the medial wall of the tympanic cavity (middle ear). This course produces a ridge known as the prominence of the facial canal (Prominentia canalis facialis), which is situated immediately superior to the vestibular window (oval window) and inferior to the prominence of the lateral semicircular canal.
• Descending (Mastoid) Segment: After reaching the posterior wall (mastoid wall) of the tympanic cavity, the nerve executes a second bend (second genu). It then runs vertically downward within the bony wall that separates the tympanic cavity from the mastoid antrum. This portion is the mastoid segment, which terminates as the nerve exits the skull through the stylomastoid foramen
It exits the cranial cavity by passing through the internal acoustic meatus.
The segments of the facial nerve within the facial canal are categorized as follows:
• Labyrinthine segment: Located within the bone, it passes superior to the vestibule of the inner ear and travels laterally to reach the medial wall of the middle ear, where it bends sharply backward at the first genu—the site of the geniculate ganglion.
• Tympanic segment: The nerve here runs horizontally backward along the medial wall of the tympanic cavity (middle ear) until it reaches the junction between the medial and posterior walls of the middle ear.
• Mastoid segment: It then descends vertically within this portion along the posterior wall of the middle ear to reach the stylomastoid foramen and exits the temporal bone.
Exiting the Skull Base and the Extracranial Segment of the Facial Nerve
Stylomastoid foramen
The facial nerve exits the skull base through this foramen, which is located between the styloid process and the mastoid process. From the foramen, the nerve loops forward to enter the facial region via the parotid gland.
In the parotid gland
After exiting the foramen, the nerve enters the posterior and then the medial aspect of the parotid gland. The facial nerve is embedded within the parotid gland.
The facial nerve is situated within the parotid gland parenchyma. Within the parotid parenchyma, the facial nerve divides into two main trunks:
• The temporofacial division, which is the superior branch.
• The cervicofacial division, which is the inferior branch. These trunks then radiate to form the parotid plexus, which gives rise to the terminal branches.
Relationship with the Mandible
The facial nerve maintains a close anatomical relationship with the neck of the mandible as it moves from the stylomastoid foramen toward the face.
• Passage: The main trunk of the facial nerve passes horizontally behind the neck of the mandible to enter the parotid parenchyma. It typically travels a distance of 5mm to 25mm before branching.
• Relationships to other structures: In this area, the facial nerve runs between the neck of the mandible and the external acoustic meatus. It lies superficial to the external carotid artery and retromandibular vein when these structures pass through or lie deep within the parotid gland.
• Clinical Significance: Because the facial nerve passes immediately posterior to the mandibular neck, mandibular condylar neck fractures or surgical interventions on the temporomandibular joint carry a risk of damaging these nerve branches.
• Temporal branches: Cross the zygomatic arch to the temporal region to innervate auricular muscles and the frontal belly of the occipitofrontalis.
• Zygomatic branches: Run across the zygomatic bone toward the orbital region to innervate the orbicularis oculi.
• Buccal branches: Run horizontally below the parotid duct to innervate the buccinator, orbicularis oris, and muscles around the nose.
• Marginal mandibular branch: Runs along or below the inferior border of the mandible to innervate the muscles of the lower lip and chin.
• Cervical branch: Descends into the neck, lying deep to the platysma, to provide its motor innervation.
A detailed understanding of muscle innervation is essential for identifying the clinical symptoms of peripheral facial nerve palsy. The overall presentation of deficits within these muscle groups allows for the accurate diagnosis of which nerve segment or branch is compromised.
The temporofacial division of the facial nerve communicates with the temporal nerve and yields numerous superficial branches in the cervicofacial region. Within the substance of the parotid gland, between its superficial and deep lobes, the temporofacial and cervicofacial divisions provide multiple interconnecting branches that constitute the parotid plexus.
• Forehead and eyelids: The frontal belly of the occipitofrontalis, the corrugator supercilii, and the orbicularis oculi.
• Infraorbital region: The zygomaticus major and zygomaticus minor.
• Nasal region: The levator labii superioris alaeque nasi, the nasalis, and the dilatator naris.
• Upper oral region: The levator labii superioris, the levator anguli oris (caninus), the buccinator, and the upper half of the orbicularis oris.
The cervicofacial division connects with the auricular branch of the cervical plexus and subsequently splits into multiple small branches, typically situated posterior and superior to the angle of the mandible.
• Chin region: The depressor anguli oris, the depressor labii inferioris, and the mentalis.
• Neck region: The platysma; this branch communicates with the transverse cervical nerve of the superficial cervical plexus.
Clinical note: Because the facial nerve divides the parotid gland into superficial and deep lobes, surgical procedures in this area, such as the excision of parotid tumors, require meticulous dissection. This is critical to avoid damaging the parotid plexus, which would result in Bell's palsy or facial muscle weakness.
Several critical anatomical relationships exist:
• External carotid artery: This vessel may be destroyed by malignant tissue or lead to significant hemorrhage during surgical procedures.
• Facial nerve (CN VII): Malignant tumors frequently cause facial paralysis; however, in cases of mixed tumors where the nerve is not yet compromised, surgical preservation of CN VII is a primary objective.
• Mandible and temporomandibular joint: Trismus occurs when a tumor infiltrates the masseter muscles or extends into the temporomandibular joint.
• External carotid artery (continued): Malignant growths can invade the arterial wall, resulting in severe bleeding.
The distribution of the facial nerve through the parotid gland exhibits several morphological patterns. The gland features a large superficial lobe and a smaller deep lobe, which are connected by an isthmus. After exiting the skull base at the stylomastoid foramen, the facial nerve travels approximately 1.25 cm before entering the deep plane of the gland just below the midpoint of its posterior border. In practice, the facial nerve enters a groove formed by the fascia of the superficial lobe. The main trunk of the nerve enters the isthmus from the posterior aspect and subsequently divides into two primary divisions: the temporofacial division superiorly, which crosses above the isthmus, and the cervicofacial division, which passes along the inferior border of the isthmus.
Because the deep lobe is small, the smaller branches located outside this lobe actually lie between the superficial lobe and the masseter muscle. During surgery, it is often observed that the temporofacial division is larger than the cervicofacial division; this is the priority branch for preservation during a parotidectomy. In certain instances, after the two primary trunks branch to encompass the superior and inferior borders of the isthmus, only a few small branches from these trunks interconnect to form a plexus immediately anterior to the isthmus.
After emerging from the skull base through the stylomastoid foramen, the facial nerve gives off its first side branches before entering the substance of the parotid gland. These branches include the following:
the posterior auricular nerve, which travels superiorly to supply the occipital belly of the occipitofrontalis and various auricular muscles.
The digastric branch provides motor innervation to the posterior belly of the digastric muscle.
The stylohyoid branch supplies the stylohyoid muscle.
Following the separation of the branches for the digastric and stylohyoid muscles, the main trunk of the facial nerve enters the posteromedial aspect of the parotid gland and begins to divide into two primary divisions—the temporofacial and cervicofacial divisions—to form the parotid plexus.
The terminal branches of the facial nerve within the facial region have been described above.
The geniculate ganglion is a sensory ganglion located deep within the petrous part of the temporal bone, specifically inside the facial canal. At this location, the facial nerve executes a sharp posterior bend known as the genu of the facial nerve. Anatomically, the ganglion contains the cell bodies of unipolar neurons that manage sensory functions, making it equivalent to the posterior root ganglion of a spinal nerve.
2. Function and Pathways
The geniculate ganglion serves as the origin for taste (special visceral afferent) fibers for the anterior two-thirds of the tongue. These peripheral fibers travel from the tongue via the lingual nerve and then join the chorda tympani to reach the ganglion. The central fibers from the geniculate ganglion form the intermediate nerve (CN VII'), which enters the brainstem to terminate in the superior portion of the solitary nucleus. Additionally, the ganglion contains neurons that receive somatic sensation from the skin of the external acoustic meatus and part of the auricle.
3. Branches Arising at the Ganglion
The greater petrosal nerve is the first branch of the facial nerve and arises directly at the geniculate ganglion. It carries presynaptic parasympathetic fibers to the pterygopalatine ganglion to provide secretomotor innervation for the lacrimal gland as well as the mucous membranes of the nasal cavity and mouth.
4. Blood Supply and Clinical Correlations
The geniculate ganglion is supplied by the petrosal branch of the middle meningeal artery. Regarding the Vagus nerve, fibers from the intermediate nerve may communicate with the auricular branch of the Vagus nerve; this pathway is considered responsible for the skin vesicles observed in Ramsay Hunt syndrome (herpes zoster oticus). Because the ganglion is situated within the petrous portion of the facial canal, temporal bone fractures or tumors such as acoustic neuromas can compress this area. Such injuries result in complete facial paralysis, loss of taste in the anterior two-thirds of the tongue, and may cause dry eye if the lesion occurs at or proximal to the origin of the greater petrosal nerve.
1. Central Lesion (Upper Motor Neuron)
This type of lesion occurs in the cerebral cortex or the internal capsule, proximal to the facial motor nucleus in the pons.
• Symptoms: Paralysis is restricted to the muscles of the lower half of the face on the side opposite the lesion.
• Explanation: The muscles of the upper face (frontal belly of the occipitofrontalis and orbicularis oculi) receive bilateral cortical innervation from both cerebral hemispheres. In contrast, the muscles of the lower face receive fibers primarily from the contralateral cortex. Consequently, a patient with a central lesion can still wrinkle their forehead and close their eyes normally on the affected side.
2. Peripheral Lesion (Lower Motor Neuron)
This occurs at the facial motor nucleus or along the nerve path after it exits the brainstem. The hallmark is complete paralysis of all muscles of facial expression on the same side as the lesion (Bell's palsy). Associated symptoms vary by segment:
• Intracranial and Internal Acoustic Meatus (IAM) Segment: The facial nerve travels alongside the vestibulocochlear nerve (CN VIII).
◦ Symptoms: Complete ipsilateral facial paralysis accompanied by deafness, tinnitus, or vertigo due to involvement of CN VIII. There is also a loss of taste, lacrimation (tearing), and salivation.
• Intratemporal Segment (Facial/Fallopian Canal): Symptoms appear cumulatively depending on which side branches are affected:
◦ Lesion proximal to the geniculate ganglion: Results in facial paralysis, dry eye (loss of the greater petrosal nerve), hyperacusis (painful sensitivity to loud sounds due to stapedius muscle paralysis), loss of taste in the anterior two-thirds of the tongue, and decreased salivation (chorda tympani involvement).
◦ Lesion distal to the geniculate ganglion but proximal to the nerve to stapedius: Lacrimation remains normal, but the patient exhibits facial paralysis, hyperacusis, loss of taste, and decreased salivation.
◦ Lesion between the nerve to stapedius and the chorda tympani: Facial paralysis and loss of taste/salivation occur. Hearing and lacrimation remain normal.
◦ Lesion at the stylomastoid foramen (after all branches have exited): Results in pure motor paralysis of the facial muscles. Taste, lacrimation, and hearing are unaffected.
3. Extracranial Segment (Within the Parotid Gland or Face)
The nerve has already divided into its terminal branches (temporal, zygomatic, buccal, marginal mandibular, and cervical).
• Symptoms: Typically results in partial paralysis or weakness of a specific group of facial muscles depending on the injured branch.
◦ Temporal/Zygomatic branches: Loss of forehead wrinkling and inability to close the eye (lagophthalmos), making the cornea vulnerable to drying and ulceration.
◦ Buccal branch: Food accumulates in the oral vestibule due to buccinator paralysis; the mouth deviates toward the healthy side.
◦ Marginal mandibular branch: Drooping of the corner of the mouth, inability to whistle, and saliva dribbling from the paralyzed side.
Summary of Typical Clinical Symptoms (Peripheral Syndrome):
• Motor: Marked facial asymmetry; natural wrinkles and folds (such as the nasolabial fold) disappear; the philtrum deviates toward the healthy side.
• Eye: Charles-Bell sign (when attempting to close the eye, the lid remains open while the eyeball rolls upward and outward).
• Sensory: Loss of taste in the anterior two-thirds of the tongue (if the lesion is proximal to the chorda tympani).
• Autonomic: Dry eye (if proximal to the geniculate ganglion) or decreased submandibular/sublingual salivation.
In the clinical examination of facial paralysis, these signs help clinicians determine if a lesion is central or peripheral, locate the specific site of injury along the nerve’s path, and suggest potential underlying causes.
ainstem (a peripheral lesion), the patient will suffer from complete facial paralysis on the same side as the injury. However, the control becomes more complex when considering the innervation descending from the cerebral cortex. 2. Innervation from the cerebral cortex to the facial motor nucleus: Complex The relationship between the Upper Motor Neuron (cortex) and the Lower Motor Neuron (pons nucleus) is not uniform for the entire face: ● The portion of the nucleus supplying the upper face (forehead, eyes): Receives corticonuclear fibers from the cerebral cortex of both hemispheres (bilateral innervation). Therefore, if the cortex on one side is damaged, the other side can compensate, allowing the patient to still wrinkle their forehead and close their eyes. ● The portion of the nucleus supplying the lower face (mouth, chin): Receives fibers only from the contralateral cerebral cortex. Clinical Significance for Differentiation: This difference is a critical landmark for diagnosing the site of a lesion: ● Central Lesion (above the nucleus in the pons): Results in paralysis only of the lower facial muscles on the contralateral side of the lesion (the upper face is spared due to bilateral innervation). ● Peripheral Lesion (at the nucleus or CN VII): Results in complete facial paralysis on the ipsilateral side of the injury. Summary: The facial nerve controls the facial muscles on the same side as its location in the pons, but the nucleus in the pons receives cortical commands from the opposite side for the lower face and from both sides for the upper face. From this, we can understand the clinical presentations of peripheral and central facial palsy syndromes when the facial nerve is compromised. Below is the translation of the clinical syndromes and diagnostic signs of facial nerve lesions into English, using precise medical terminology based on the provided sources:
Facial nerve: anatomy and surgical anatomy.
The facial nerve (CN VII) is a mixed nerve containing motor, sensory, and autonomic (parasympathetic) fibers. Its course is highly complex, extending from the brainstem, traversing the temporal bone, and terminating in the muscles of the face.
The facial nerve (CN VII) is a mixed nerve containing motor, sensory, and autonomic (parasympathetic) fibers. Its course is highly complex, extending from the brainstem, traversing the temporal bone, and terminating in the muscles of the face.
Origins and Emergence
• Real Origins (Nuclei):◦ Facial motor nucleus: Located in the pons. Motor fibers supply the ipsilateral muscles of facial expression (they do not decussate after leaving the nucleus).
◦ Superior salivatory nucleus and Lacrimal nucleus: Provide parasympathetic innervation.
◦ Sensory fibers for taste terminate in the solitary nucleus.
• Apparent Origin: The nerve emerges from the brainstem at the pontomedullary junction (bulbopontine sulcus).
• The facial nerve emerges as two roots: a large motor root located medially and a smaller intermediate nerve (CN VII') located laterally.
Intracranial and Intratemporal Segments
This first portion is often referred to as the labyrinthine segment.• In the posterior cranial fossa: From the brainstem, the nerve travels laterally and forward to reach the temporal bone.
• Internal acoustic meatus (IAM): The two roots of the facial nerve enter this opening along with the vestibulocochlear nerve (CN VIII) and the labyrinthine artery (which is a branch of the anterior inferior cerebellar artery - AICA).
• The blood supply to this region is provided by the labyrinthine artery.
Within the internal auditory meatus (IAM), the nervus intermedius merges with the motor root to establish a unified trunk. This combined facial nerve complex is situated in the anterosuperior quadrant of the meatus. Within this trunk, a specific orientation is maintained: the motor fibers are positioned anteriorly, while the nervus intermedius fibers lie posteriorly.
Anatomical Landmarks and Compartmentalization
As the nerve reaches the lateral extremity (fundus) of the meatus, it is partitioned from adjacent cranial nerves by two distinct ridges:
• The Transverse (Falciform) Crest: A horizontal partition composed of dura and sometimes bone. It serves as the boundary separating the facial nerve (above) from the cochlear nerve (below).
• Bill’s Bar (Vertical Crest): An incomplete vertical ridge of bone and dura. This landmark separates the facial nerve (anteriorly) from the superior vestibular nerve (posteriorly).
image: internal acoustic meatus
Blood supply: labyrinthine artery - brand of the anterior inferior cerebellar artery.
Intratemporal Segments of the Facial Nerve
• Facial Canal Segment: At the fundus of the internal acoustic meatus, the nerve enters a separate passage called the facial canal. This first portion, often called the labyrinthine segment, runs between the vestibule and the cochlea until it expands to form the Geniculate ganglion.• Genu of the Facial Nerve (First Genu): At the geniculate ganglion, the nerve makes a sharp, knee-like bend as it turns abruptly posterior.
• Tympanic Segment: Following the genu, the nerve creates a horizontal portion on the medial wall of the tympanic cavity (middle ear). This course produces a ridge known as the prominence of the facial canal (Prominentia canalis facialis), which is situated immediately superior to the vestibular window (oval window) and inferior to the prominence of the lateral semicircular canal.
• Descending (Mastoid) Segment: After reaching the posterior wall (mastoid wall) of the tympanic cavity, the nerve executes a second bend (second genu). It then runs vertically downward within the bony wall that separates the tympanic cavity from the mastoid antrum. This portion is the mastoid segment, which terminates as the nerve exits the skull through the stylomastoid foramen
It exits the cranial cavity by passing through the internal acoustic meatus.
The segments of the facial nerve within the facial canal are categorized as follows:
• Labyrinthine segment: Located within the bone, it passes superior to the vestibule of the inner ear and travels laterally to reach the medial wall of the middle ear, where it bends sharply backward at the first genu—the site of the geniculate ganglion.
• Tympanic segment: The nerve here runs horizontally backward along the medial wall of the tympanic cavity (middle ear) until it reaches the junction between the medial and posterior walls of the middle ear.
• Mastoid segment: It then descends vertically within this portion along the posterior wall of the middle ear to reach the stylomastoid foramen and exits the temporal bone.
Facial nerve lesion signs and clinical signs.
The diagram below provides a schematic of the segments and specific regions where lesions result in distinct clinical presentations.
Based on the merging and branching patterns, lesions in different segments of the facial nerve produce cumulative deficits; the further centrally (proximally) the lesion is located, the more severe the clinical symptoms become.Exiting the Skull Base and the Extracranial Segment of the Facial Nerve
Stylomastoid foramen
The facial nerve exits the skull base through this foramen, which is located between the styloid process and the mastoid process. From the foramen, the nerve loops forward to enter the facial region via the parotid gland.
In the parotid gland
After exiting the foramen, the nerve enters the posterior and then the medial aspect of the parotid gland. The facial nerve is embedded within the parotid gland.
Relationships of the facial nerve at the parotid gland.
In the parotid region, the nerve lies superficial to the retromandibular vein and the external carotid artery.The facial nerve is situated within the parotid gland parenchyma. Within the parotid parenchyma, the facial nerve divides into two main trunks:
• The temporofacial division, which is the superior branch.
• The cervicofacial division, which is the inferior branch. These trunks then radiate to form the parotid plexus, which gives rise to the terminal branches.
Relationship with the Mandible
The facial nerve maintains a close anatomical relationship with the neck of the mandible as it moves from the stylomastoid foramen toward the face.
• Passage: The main trunk of the facial nerve passes horizontally behind the neck of the mandible to enter the parotid parenchyma. It typically travels a distance of 5mm to 25mm before branching.
• Relationships to other structures: In this area, the facial nerve runs between the neck of the mandible and the external acoustic meatus. It lies superficial to the external carotid artery and retromandibular vein when these structures pass through or lie deep within the parotid gland.
• Clinical Significance: Because the facial nerve passes immediately posterior to the mandibular neck, mandibular condylar neck fractures or surgical interventions on the temporomandibular joint carry a risk of damaging these nerve branches.
Terminal Branches of the Facial Nerve
The facial nerve emerges at the anterior border of the parotid gland and divides into five main groups of branches to provide motor innervation to the muscles of facial expression:• Temporal branches: Cross the zygomatic arch to the temporal region to innervate auricular muscles and the frontal belly of the occipitofrontalis.
• Zygomatic branches: Run across the zygomatic bone toward the orbital region to innervate the orbicularis oculi.
• Buccal branches: Run horizontally below the parotid duct to innervate the buccinator, orbicularis oris, and muscles around the nose.
• Marginal mandibular branch: Runs along or below the inferior border of the mandible to innervate the muscles of the lower lip and chin.
• Cervical branch: Descends into the neck, lying deep to the platysma, to provide its motor innervation.
A detailed understanding of muscle innervation is essential for identifying the clinical symptoms of peripheral facial nerve palsy. The overall presentation of deficits within these muscle groups allows for the accurate diagnosis of which nerve segment or branch is compromised.
The temporofacial division of the facial nerve communicates with the temporal nerve and yields numerous superficial branches in the cervicofacial region. Within the substance of the parotid gland, between its superficial and deep lobes, the temporofacial and cervicofacial divisions provide multiple interconnecting branches that constitute the parotid plexus.
The terminal branches reach the following muscle groups
• Temporal region: The auricularis anterior and the muscles on the anterior surface of the auricle.• Forehead and eyelids: The frontal belly of the occipitofrontalis, the corrugator supercilii, and the orbicularis oculi.
• Infraorbital region: The zygomaticus major and zygomaticus minor.
• Nasal region: The levator labii superioris alaeque nasi, the nasalis, and the dilatator naris.
• Upper oral region: The levator labii superioris, the levator anguli oris (caninus), the buccinator, and the upper half of the orbicularis oris.
The cervicofacial division connects with the auricular branch of the cervical plexus and subsequently splits into multiple small branches, typically situated posterior and superior to the angle of the mandible.
The terminal branches of this division include:
• Lower oral region: The risorius and the lower half of the orbicularis oris.• Chin region: The depressor anguli oris, the depressor labii inferioris, and the mentalis.
• Neck region: The platysma; this branch communicates with the transverse cervical nerve of the superficial cervical plexus.
Clinical note: Because the facial nerve divides the parotid gland into superficial and deep lobes, surgical procedures in this area, such as the excision of parotid tumors, require meticulous dissection. This is critical to avoid damaging the parotid plexus, which would result in Bell's palsy or facial muscle weakness.
Surgical Anatomy of the Parotid Gland and Facial Nerve Relations
The parotid gland is relatively extensive and deep, stretching from the zygoma to the angle of the mandible, from the anterosuperior aspect of the sternocleidomastoid muscle to the masseter muscle, and from the cervical fascia to the pharynx. Consequently, tumors of this gland often spread extensively and deeply.Several critical anatomical relationships exist:
• External carotid artery: This vessel may be destroyed by malignant tissue or lead to significant hemorrhage during surgical procedures.
• Facial nerve (CN VII): Malignant tumors frequently cause facial paralysis; however, in cases of mixed tumors where the nerve is not yet compromised, surgical preservation of CN VII is a primary objective.
• Mandible and temporomandibular joint: Trismus occurs when a tumor infiltrates the masseter muscles or extends into the temporomandibular joint.
• External carotid artery (continued): Malignant growths can invade the arterial wall, resulting in severe bleeding.
Applied Surgical Anatomy of the Parotid Gland
In 1937, the parotid gland was first described as consisting of two lobes. The facial nerve does not lie within the actual parenchyma of the gland; instead, it passes through the gland between the two lobes in a "sandwich clamp" fashion. The branches traversing the gland are motor branches and do not contain any secretomotor fibers. As is generally understood, no secretory gland in the body contains lymph nodes within its actual parenchyma; components such as lymph nodes and nerves are situated outside the glandular tissue proper.The distribution of the facial nerve through the parotid gland exhibits several morphological patterns. The gland features a large superficial lobe and a smaller deep lobe, which are connected by an isthmus. After exiting the skull base at the stylomastoid foramen, the facial nerve travels approximately 1.25 cm before entering the deep plane of the gland just below the midpoint of its posterior border. In practice, the facial nerve enters a groove formed by the fascia of the superficial lobe. The main trunk of the nerve enters the isthmus from the posterior aspect and subsequently divides into two primary divisions: the temporofacial division superiorly, which crosses above the isthmus, and the cervicofacial division, which passes along the inferior border of the isthmus.
Because the deep lobe is small, the smaller branches located outside this lobe actually lie between the superficial lobe and the masseter muscle. During surgery, it is often observed that the temporofacial division is larger than the cervicofacial division; this is the priority branch for preservation during a parotidectomy. In certain instances, after the two primary trunks branch to encompass the superior and inferior borders of the isthmus, only a few small branches from these trunks interconnect to form a plexus immediately anterior to the isthmus.
After emerging from the skull base through the stylomastoid foramen, the facial nerve gives off its first side branches before entering the substance of the parotid gland. These branches include the following:
the posterior auricular nerve, which travels superiorly to supply the occipital belly of the occipitofrontalis and various auricular muscles.
The digastric branch provides motor innervation to the posterior belly of the digastric muscle.
The stylohyoid branch supplies the stylohyoid muscle.
Following the separation of the branches for the digastric and stylohyoid muscles, the main trunk of the facial nerve enters the posteromedial aspect of the parotid gland and begins to divide into two primary divisions—the temporofacial and cervicofacial divisions—to form the parotid plexus.
The terminal branches of the facial nerve within the facial region have been described above.
Geniculate Ganglion of the Facial Nerve
1. Location and StructureThe geniculate ganglion is a sensory ganglion located deep within the petrous part of the temporal bone, specifically inside the facial canal. At this location, the facial nerve executes a sharp posterior bend known as the genu of the facial nerve. Anatomically, the ganglion contains the cell bodies of unipolar neurons that manage sensory functions, making it equivalent to the posterior root ganglion of a spinal nerve.
2. Function and Pathways
The geniculate ganglion serves as the origin for taste (special visceral afferent) fibers for the anterior two-thirds of the tongue. These peripheral fibers travel from the tongue via the lingual nerve and then join the chorda tympani to reach the ganglion. The central fibers from the geniculate ganglion form the intermediate nerve (CN VII'), which enters the brainstem to terminate in the superior portion of the solitary nucleus. Additionally, the ganglion contains neurons that receive somatic sensation from the skin of the external acoustic meatus and part of the auricle.
3. Branches Arising at the Ganglion
The greater petrosal nerve is the first branch of the facial nerve and arises directly at the geniculate ganglion. It carries presynaptic parasympathetic fibers to the pterygopalatine ganglion to provide secretomotor innervation for the lacrimal gland as well as the mucous membranes of the nasal cavity and mouth.
4. Blood Supply and Clinical Correlations
The geniculate ganglion is supplied by the petrosal branch of the middle meningeal artery. Regarding the Vagus nerve, fibers from the intermediate nerve may communicate with the auricular branch of the Vagus nerve; this pathway is considered responsible for the skin vesicles observed in Ramsay Hunt syndrome (herpes zoster oticus). Because the ganglion is situated within the petrous portion of the facial canal, temporal bone fractures or tumors such as acoustic neuromas can compress this area. Such injuries result in complete facial paralysis, loss of taste in the anterior two-thirds of the tongue, and may cause dry eye if the lesion occurs at or proximal to the origin of the greater petrosal nerve.
Symptoms of Facial Nerve Lesions Across Different Segments
The clinical manifestations of facial nerve (CN VII and CN VII') lesions depend on the specific anatomical location of the injury along its complex pathway from the center to the periphery. Lesions can be categorized into several levels:1. Central Lesion (Upper Motor Neuron)
This type of lesion occurs in the cerebral cortex or the internal capsule, proximal to the facial motor nucleus in the pons.
• Symptoms: Paralysis is restricted to the muscles of the lower half of the face on the side opposite the lesion.
• Explanation: The muscles of the upper face (frontal belly of the occipitofrontalis and orbicularis oculi) receive bilateral cortical innervation from both cerebral hemispheres. In contrast, the muscles of the lower face receive fibers primarily from the contralateral cortex. Consequently, a patient with a central lesion can still wrinkle their forehead and close their eyes normally on the affected side.
2. Peripheral Lesion (Lower Motor Neuron)
This occurs at the facial motor nucleus or along the nerve path after it exits the brainstem. The hallmark is complete paralysis of all muscles of facial expression on the same side as the lesion (Bell's palsy). Associated symptoms vary by segment:
• Intracranial and Internal Acoustic Meatus (IAM) Segment: The facial nerve travels alongside the vestibulocochlear nerve (CN VIII).
◦ Symptoms: Complete ipsilateral facial paralysis accompanied by deafness, tinnitus, or vertigo due to involvement of CN VIII. There is also a loss of taste, lacrimation (tearing), and salivation.
• Intratemporal Segment (Facial/Fallopian Canal): Symptoms appear cumulatively depending on which side branches are affected:
◦ Lesion proximal to the geniculate ganglion: Results in facial paralysis, dry eye (loss of the greater petrosal nerve), hyperacusis (painful sensitivity to loud sounds due to stapedius muscle paralysis), loss of taste in the anterior two-thirds of the tongue, and decreased salivation (chorda tympani involvement).
◦ Lesion distal to the geniculate ganglion but proximal to the nerve to stapedius: Lacrimation remains normal, but the patient exhibits facial paralysis, hyperacusis, loss of taste, and decreased salivation.
◦ Lesion between the nerve to stapedius and the chorda tympani: Facial paralysis and loss of taste/salivation occur. Hearing and lacrimation remain normal.
◦ Lesion at the stylomastoid foramen (after all branches have exited): Results in pure motor paralysis of the facial muscles. Taste, lacrimation, and hearing are unaffected.
3. Extracranial Segment (Within the Parotid Gland or Face)
The nerve has already divided into its terminal branches (temporal, zygomatic, buccal, marginal mandibular, and cervical).
• Symptoms: Typically results in partial paralysis or weakness of a specific group of facial muscles depending on the injured branch.
◦ Temporal/Zygomatic branches: Loss of forehead wrinkling and inability to close the eye (lagophthalmos), making the cornea vulnerable to drying and ulceration.
◦ Buccal branch: Food accumulates in the oral vestibule due to buccinator paralysis; the mouth deviates toward the healthy side.
◦ Marginal mandibular branch: Drooping of the corner of the mouth, inability to whistle, and saliva dribbling from the paralyzed side.
Summary of Typical Clinical Symptoms (Peripheral Syndrome):
• Motor: Marked facial asymmetry; natural wrinkles and folds (such as the nasolabial fold) disappear; the philtrum deviates toward the healthy side.
• Eye: Charles-Bell sign (when attempting to close the eye, the lid remains open while the eyeball rolls upward and outward).
• Sensory: Loss of taste in the anterior two-thirds of the tongue (if the lesion is proximal to the chorda tympani).
• Autonomic: Dry eye (if proximal to the geniculate ganglion) or decreased submandibular/sublingual salivation.
In the clinical examination of facial paralysis, these signs help clinicians determine if a lesion is central or peripheral, locate the specific site of injury along the nerve’s path, and suggest potential underlying causes.
ainstem (a peripheral lesion), the patient will suffer from complete facial paralysis on the same side as the injury. However, the control becomes more complex when considering the innervation descending from the cerebral cortex. 2. Innervation from the cerebral cortex to the facial motor nucleus: Complex The relationship between the Upper Motor Neuron (cortex) and the Lower Motor Neuron (pons nucleus) is not uniform for the entire face: ● The portion of the nucleus supplying the upper face (forehead, eyes): Receives corticonuclear fibers from the cerebral cortex of both hemispheres (bilateral innervation). Therefore, if the cortex on one side is damaged, the other side can compensate, allowing the patient to still wrinkle their forehead and close their eyes. ● The portion of the nucleus supplying the lower face (mouth, chin): Receives fibers only from the contralateral cerebral cortex. Clinical Significance for Differentiation: This difference is a critical landmark for diagnosing the site of a lesion: ● Central Lesion (above the nucleus in the pons): Results in paralysis only of the lower facial muscles on the contralateral side of the lesion (the upper face is spared due to bilateral innervation). ● Peripheral Lesion (at the nucleus or CN VII): Results in complete facial paralysis on the ipsilateral side of the injury. Summary: The facial nerve controls the facial muscles on the same side as its location in the pons, but the nucleus in the pons receives cortical commands from the opposite side for the lower face and from both sides for the upper face. From this, we can understand the clinical presentations of peripheral and central facial palsy syndromes when the facial nerve is compromised. Below is the translation of the clinical syndromes and diagnostic signs of facial nerve lesions into English, using precise medical terminology based on the provided sources: