Autoimmune inner ear disease (AIED)
Post date: 18/09/2023
What is Autoimmune inner ear disease (AIED)?
Autoimmune inner ear disease (AIED) is a rare disease cause Hearing loss problem.Autoimmune inner ear disease (AIED) has been defined as a condition of bilateral Sensorineural hearing loss (SNHL), caused by an ‘uncontrolled’ immune system response.
The inner ear can be the direct target of the immune response, but it can be additionally damaged by a deposition of circulating immune complexes or by systemic immune-mediated diseases.
A simpler explains:
Autoimmune inner ear disease (AIED) is a type of sensorineural hearing loss, starting at one ear and hearing loss progresses rapidly to both ears.
Who is likely to have Autoimmune inner ear disease (AIED)?
Autoimmune inner ear disease AIED most commonly affects people between the ages of 30 and 60, and it is slightly more common in women than in men, the risk is highest in age 20 to 50.People may have other autoimmune diseases coexisting disease and condition along with Autoimmune inner ear disease AIED:
- lupus
- rheumatoid arthritis
- scleroderma
- ulcerative colitis
- Tinnitus, Cogan’s syndrome, relapsing polychondritis, systemic lupus erythematosus, Wegener’s granulomatosis, polyarteritis nodosa, Sjogren’s syndrome, and Lyme disease.
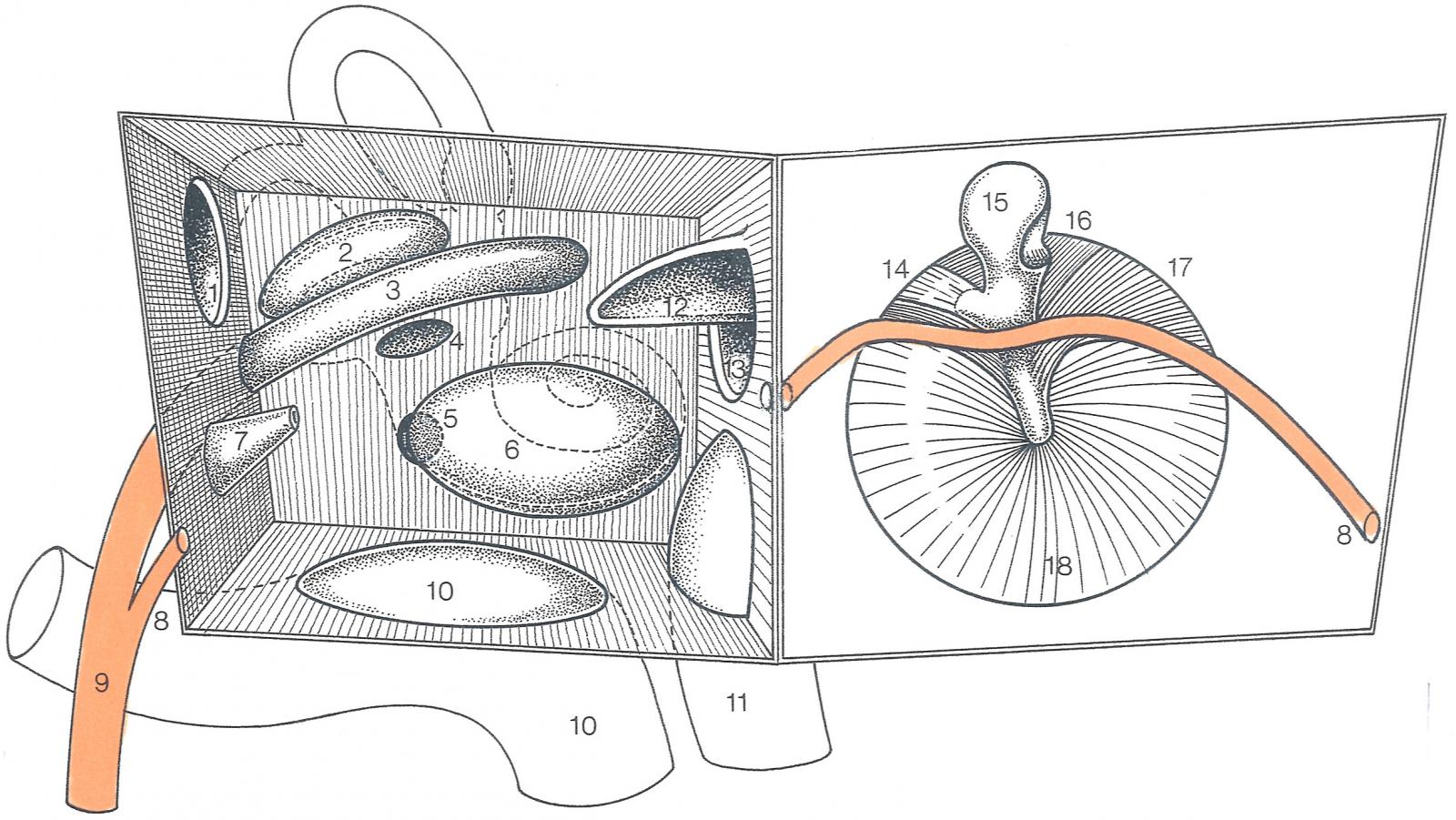
Pathogenesis of Autoimmune inner ear disease AIED
The onset of Autoimmune inner ear disease (AIED) is between 3 and 90 days. Cochlear symptoms can be associated with vestibular disorders and in 15%–30% of cases, AIED occurs in the contest of a systemic autoimmune disease.Currently, the onset of immune-mediated SNHL is not a well-understood process and the pathogenetic mechanisms of AIED remain unclear.
An uncontrolled attack against inner ear antigens, resulting in both T-cell responses and autoantibody development, has been proposed as the pathogenetic mechanism of AIED. This immunological process may result in cochlear and vestibular insults. The most commonly reported endocochlear damages are cochlear vasculitis, atrophy of the organ of Corti, otic capsule otospongiosis, endolymphatic hydrops and spiral ganglion degeneration.
Data in the literature suggest that the endolymphatic sac could be primarily involved in the pathogenesis of Autoimmune inner ear disease AIED.
Many antigens in the inner ear and possibly in the endolymphatic sac have been recognized as possible AIED targets. Among those, cochlin, an extracellular matrix protein specifically present in the inner ear, has been proposed as a possible cochlear antigen involved in the pathogenetic mechanism of AIED: anti-cochlin antibodies have been detected in a small cohort of patients affected by Autoimmune inner ear disease (AIED) and may advocate a cochlear specific antibody response.
After the activation of the immune response and the release of interleukin (IL)-1β, the autoimmune response is promoted and the activated circulating leukocytes and immunoglobulins can target, by chemotaxis, the inner ear in response to antigenic stimuli. The activated lymphocytes cross the blood-labyrinthine barrier (probably entering the cochlea along the spiral modiolar vein of the scala tympani) and reach the endolymphatic sac.
Tumor necrosis factor (TNF) is also considered a pro-inflammatory cytokine promoting the autoimmune response.
Symptoms of Autoimmune inner ear disease (AIED)
The main symptoms of AIED are sensorineural Hearing loss symptoms that happen in one ear progressing rapidly to the second ear.Hearing loss
The symptoms Autoimmune inner ear disease of AIED can vary from person to person. The clinical expression of AIED can be heterogeneous, but in most cases (80%) patients show a 30 dB, or higher, one or both ear SNHL.
Sudden hearing loss in one ear that progresses to the ear over time, The onset of AIED is between 3 and 90 days. Hearing loss might cause threshold changes at times.
In some cases, the hearing loss profile shows a conductive component (in approximately 33% of patients affected by granulomatosis with polyangiitis, a conductive hearing loss could be caused by the involvement of the Eustachian tube and/or the middle ear mucosa).
Tinnitus (ringing, roaring, or hissing in the ears). In 25%–50% of cases, tinnitus and ear fullness can also be present.
Fullness in the ear.
Dizziness, Vertigo or problems with balance, feel like you're spinning. In about 50% of the Autoimmune inner ear disease AIED patients, hearing loss is also associated with vestibular symptoms, such as imbalance and motion intolerance, ataxia and positional or episodic vertigo.
Other systemic Common symptoms of autoimmune disease include:
- Fatigue.
- Joint pain and swelling.
- Skin problems.
- Abdominal pain or digestive issues.
- Recurring fever.
- Swollen glands.
Frequently, in the early stage of AIED, only one ear is affected.
The diagnosis of Autoimmune inner ear disease AIED
There are no standardized diagnostic criteria or reliable diagnostic tests for the diagnosis of Autoimmune inner ear disease (AIED) yet.The definition of immune-mediated cochleovestibular disorders is a challenging diagnosis based on exclusion.
The symptoms of Autoimmune inner ear disease AIED mimic other ear disorders so diagnosis of Autoimmune inner ear disease (AIED) can be difficult.
Diagnosis of Autoimmune inner ear disease AIED is often mistaken for otitis media until the patient develops a loss in the second ear.
Relate topic:
The different between Autoimmune inner ear disease (AIED) and otitis media.
One diagnostic test that is promising is the Western blot immunoassay.
The definition of immune-mediated cochleovestibular disorders is a challenging diagnosis based on exclusion.
Doctors typically diagnose Autoimmune inner ear disease AIED after all other probable causes for symptoms have been ruled out.
If you have unexplained hearing loss that is progressing in both ears over a period of weeks, consult an ear, nose, and throat (ENT) specialist.
You will very certainly be subjected to the following tests:
Serial audiograms assess your hearing over the course of several months.
Imaging studies, such as MRIs, can reveal features of the inner ear structure and help rule out other cochlear issues.
Vestibular testing might put your equilibrium to the test. This examination could last several hours.
A blood test is another crucial screening. This test looks for increased amounts of T lymphocytes in the inner ear that respond to antigens.
What causes Autoimmune inner ear disease (AIED)?
The exact cause of autoimmune inner ear disease (AIED) is unknown.Genetic factors may also play a role in AIED. People who have a family history of autoimmune diseases are more likely to develop AIED.
A mix of genetic and environmental factors is thought to be responsible. Some of the environmental factors that may trigger AIED include:
Viral infections: Some viruses, such as the Epstein-Barr virus, have been linked to AIED.
Head injuries: Head injuries that damage the inner ear may trigger an autoimmune response.
Exposure to certain chemicals: Exposure to certain chemicals, such as those used in chemotherapy, may also trigger an autoimmune response.
Treatment for Autoimmune inner ear disease (AIED)
The treatment for AIED is often individualized and may vary depending on the severity of the disease and the patient's response to treatment, depending on some factors.The severity of symptoms
- Age
- Lifestyle
- Health issues
- Medication tolerance.
Medication treatment for Autoimmune inner ear disease (AIED)
Currently, there are no consensus treatment recommendations for management of AIED.A review in 2020 created a novel treatment protocol based on existing evidence.
- Oral steroid
- Nonsteroidal immunosuppressants
- Intratympanic steroid
- Biologic
Oral steroids
Oral steroids is the first‐line treatment for AIED.The audiologic improvement in 28 (44%) and 11 (71.4%) patients treated with oral steroids, respectively.
In a 2005 study, 116 patients were treated with a 1‐month course of oral prednisone (60 mg/day), during which time they underwent serial audiometry. Sixty‐nine (59.5%) of these patients showed improvements in word indication score (WIS) ranging from 2‐80% and 62 (53.5%) patients showed 1 dB or more improvement in pure tone averages.
Side effects from corticosteroids can include:
- Fluid retention and weight gain
- High blood pressure, high blood glucose index
- Mood swings
- Headaches, stomach ache
- Nausea
Intratympanic steroids
If your treatment with oral steroids is not improved or cannot tolerate long‐term treatment. Then, Intratympanic (IT) steroid injections will be used to treat AIED.Side effects associated with IT steroids are much fewer than oral steroids and include transient:
- Dizziness,
- injection site pain
- Vertigo
- tongue numbness, and a small perforation of the tympanic membrane.
Nonsteroidal immunosuppressants
Cyclophosphamide exerts its effects through the alkylation of DNA, inhibiting protein synthesis.cyclophosphamide in conjunction with steroids for treatment of AIED with promising results, demonstrating an average 15 dB pure tone improvement and 20% speech discrimination score improvement.
Since this time, studies have been limited and data has shown poor results in hearing improvement with cyclophosphamide.
Cyclophosphamide is no longer frequently used to treat AIED due to its side effect profile which includes gonadal, bladder, and bone marrow toxicity.
Methotrexate is used as an alternative treatment for refractory AIED;
Methotrexate works by inhibiting the enzyme dihydrofolate reductase, preventing the synthesis of nucleotides necessary for DNA and RNA formation.
Methotrexate has better long‐term tolerability than cyclophosphamide;
The most common side effects are nausea, vomiting, and mucosal ulcers.
The major adverse effect of methotrexate is hepatotoxicity, which can be prevented with folic acid supplementation.
Treatment outcomes have varied with hearing improvement ranging from 0% to 70%.
Methotrexate appears to be more efficacious in treating vestibular symptoms with reported subjective improvements in 80% to 100% of patients.
Biologics
To treat AIED, Multiple biologic agents have been used.TNF‐α is a proinflammatory cytokine that has been targeted by several drugs including the following: etanercept, infliximab, golimumab, and adalimumab. These drugs are generally well tolerated.
Rituximab is a monoclonal antibody directed against the CD20 B‐cell antigen, exerting cytotoxic effects against B‐cells and preventing antibody formation.
Rituximab has been used to treat steroid refractory AIED and common side effects include:
- Transfusion reaction
- Cytopenias
- Headache
- Hair loss.
Three of these subjects relapsed upon discontinuation of treatment and their relapse was correlated with increased plasma IL‐1β levels.
The drug was well tolerated and side effects were limited to injection site reactions.
Other potential side effects of Anakinra include nausea, diarrhea, headache, sore throat, and congestion.
Biologics may present a heightened risk of infection because of the way the drugs work on the immune system.
Hearing device: Cochlear implant and hearing aids
Auditory devices may help you manage hearing loss caused by AIED. These can either heighten or improve your hearing.A cochlear implant
A cochlear implant is a small electronic device that stimulates the cochlear nerve to improve hearing. The implant consists of an internal component that inserts into the inner ear and an exterior component that is situated behind the ear. Cochlear implants are often reserved for patients of severe hearing loss or specific hearing loss patterns.
Hearing aids.
Hearing aids are devices that amplify sound so that it can be detected by the ear. They are worn behind the ear or in the ear canal. Hearing aids are typically used for people with mild to moderate hearing loss.
For many persons with AIED, hearing aids are also affordable alternatives. They are less invasive than cochlear implants and much cheaper.
The best way to decide which device is right for you is to talk to a doctor or audiologist. They can assess your hearing loss and recommend the best treatment option for you
Dr. Nguyen Minh.
I hope this information is helpful. Please let me know if you have any other questions. Thank you!